

My mind is a convoluted dark place. I tend to gravitate toward the glass being half empty. I do not think highly of myself. I’m convinced that everyone else considers me worthless as well. As a teenager, this negative cognitive distortion of mine, was diagnosed as Clinically Depressed. A common label for back then, that in today’s ever evolving psychiatric terminology, has been upgraded to the more severe sounding Major Depressive Disorder (MDD). Or in cases where it just doesn’t ever get better, Persistent Depressive Disorder, or simply Dysthymia. The official definition is either “a serious, common mood disorder characterized by persistent, intense feelings of sadness,” or “a chronic depression lasting for two or more years.”
When I say, “in my teens,” I’m referring to over fifty years ago. Which is much longer than “two or more years,” and I’ve been continually plagued by “intense feelings of sadness” my entire life. Which is my long-winded way of saying I’ve been navigating depression; major, severe, persistent, clinical, whatever, for a very long time. At this point, one would think I’d be accustomed to getting up in the morning with the ever-prevailing thoughts of what’s the point to all this? and why even try? Or I’d have somehow come to terms with finding little to no joy in this world. Regrettably that’s not the case. Every day feels like another disastrous excursion into futility, an epic overwhelming battle of willpower, or once again, having to drag my ass out of one more sordid pit of despair—only to repeat it all again the next day.
Yet it’s not like I just sit around wallowing in this wretched pool of hopelessness. I don’t want to be despondent. I want to believe there’s goodness in this world. I rather not be a blackhole of sorrow. And though I’d love to be magically relieved of this prolonged misery—I mean that would be nice—I know it won’t just miraculously happen. In an effort to right this chemical imbalance in my brain, I routinely engage in daily activities that theoretical are reported to help. Every morning I scramble to orchestrate the right combination of stimulants (in my case caffeine), produce the needed endorphins (copious amounts of exercise), invite in the desired serotonin (daily meditation), and stock up on dopamine (a diet rich in tyrosine which should include, meats, dairy, nuts, seeds, and soy). Only I’m a vegetarian and I’m allergic to soy—so this one is always challenging.
Unfortunately, the hard part, even with all that, is my brain’s chemistry isn’t always agreeable. Some days all goes as planned and I can manage a somewhat “positive” outlook. Other days, it doesn’t matter what I do, the nagging urge to just go back to bed and pull the covers over my head, readily appears to be the only rational response.
Because the above solution is a complicated practice (and a lot of work), and took me years to actually implement into a routine-like-schedule. I have to admit that for the majority of my life I took the “easier” way out, and self-medicated; starting with alcohol, marijuana, psychedelics, tranquilizers, amphetamines, benzodiazepines, antispasmodics, sedatives, stimulants, and finally opiates. Utilizing these “controlled substances” I was able to manipulate my brain chemistry and as long as I was under the influence, for the most part, anyway—all was well. The unfortunate consequences being that said drugs are illegal (hey there, Johnny law), it takes more and more to achieve the same results (goodbye financial security), and the unscrupulous importers and manufacturers of said drugs are not all that discerning with what’s in the drugs—and that includes pharmaceutical companies as well as cartels (come on in anaphylaxis and lung disease).
Cocaine and heroin are notorious for being cut with “benign” substances that contain anywhere from thirty to sixty percent sugar (oh, hello diabetes). Meth is derived from caustic and/or toxic chemicals such as phosphorus, sulfur, ephedrine, pseudoephedrine, copper salts, and rinsed with acetone (corrosive cardiovascular disease, anyone?). Cocaine is processed with solvents such as diesel fuel and kerosene and contains fillers like Levamisole; a veterinary medicine used to treat parasites in livestock. Or Benzocaine; a local anesthetic that causes raspatory issues (goodbye tapeworms and hello pneumonia). And the majority of the “cooks” making these drugs are not trained chemists, or even high school chemistry teachers a la Breaking Bad. None of these wannabe-pharmacologists care if the final process doesn’t quite wash out the impurities. Meanwhile we addicts blissfully shoot them into our veins, gleefully swallowing “bootleg” pills, and greedily suck their pungent smoke into our lungs—and our body chemistry goes haywire. Not just the haywire we were hoping for. And the long-term effects are devastating.
Brain chemicals that should have lasted well into our “golden years” eventually become depleted. Extended durations of using drugs that mimic our natural neurochemicals creates an unprecedented production overload and the body just stops producing them. The synapses in our brains become burned out from overuse, they over-fire, mis-fire, stop firing, or just close up shop and go out of business—our dopamine, serotonin, and endorphins taking a permanent holiday. A prolonged and profusive use of meth and cocaine can cause psychosis—a loss of contact with reality—as well as facial tics, contortions, confusion, and paranoia; that some users don’t fully come back from. While heroin and its younger sister fentanyl prefer to just outright kill you, or bring you so close to death’s door with an overdose, it irreversibly destroys brain cells in the process.
Late at night, when I can’t sleep, staring at the ceiling, I ruminate on the “lucky ones” who succumbed to a fatal overdose—a final lethal high relieving them of this daily despair. Having overdosed on heroin eight times (brought back by numerous doses of Narcan), I’ve experienced a majority of this aftermath and residual fallout I’ve previously mentioned. Even though it’s been many years since I’ve injected anything into my system, my body and mind are still complaining, “what the fuck did you do, dude.” Now in my sixties and drug free, my brain chemistry is a daily free-for-all. I never know what I’m going to get. It’s a mental crap shoot. I may be depressed, or so goddamn anxious I can’t even leave the house.

This has led me to seeking help from psychiatrists and big pharma (hey, it’s the only game in town), and that has created a whole other predicament—rife with its own set of problems. But, at this point, what else am I going to do?
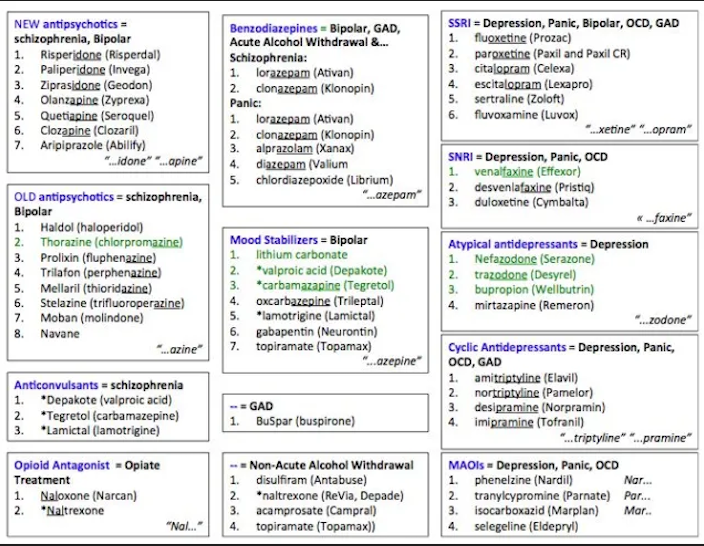
In response to a major portion of the world’s population experiencing mental health issues (one in five adults suffer some form of mental illness), the pharmaceutical industry has concocted a dazzling array of antidepressants, anti-anxieties, stimulants, and mood stabilizers. Gone are the days of Prozac and valium being the universal cure. Now-a-days-there are serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs) atypical antidepressants, as well as the SSRIs (selective serotonin reuptake inhibitors), and apparently, more on the way every day. Mental health is big business. The global antidepressant market is an ever growing eighteen-billion-dollar industry.
However, what isn’t so readily advertised is what these drugs actually do (besides what the pharmacologists think they should do). They don’t really know what happens when you change a person’s brain chemistry. Sure, the drugs may help with the problem. But what else are they doing? The prevailing party line is your psychiatrist has deemed that your declining mental health outweighs any adverse reactions. Do you want to be suicidal, or experience explosive diarrhea? Your choice. Except your doctor isn’t the one taking these meds; and all of these drugs, and I do mean all of them, have known side effects. Weight gain, nausea, drowsiness, dizziness, nausea, headaches, sleepiness, constipation, anxiety, and sexual dysfunction—just to name a few.
Because what they do know is when you mess with the brain’s chemistry (just like when someone is using excessive amounts of narcotics), the body stop producing its natural hormones, gets lazy and stops firing our brain synapses, or our neurotransmitters get disrupted; and when you increase, or decrease, the normal amounts (or decide how the brain takes them in), weird unpredictable stuff happens.
For the last eleven years I’ve been prescribed a fairly common norepinephrine-dopamine reuptake inhibitor (NDRI) for depression and anxiety, with little to no side effects. At least for me that was true—but everyone’s brain chemistry is different—and for a while there I chugged along like a little happy medicated choo-choo (on a good day that is). Until one day I was at work and someone said something that annoyed me, and this intense rage irrupted throughout my body and mind. My chest muscles tensed, my temple throbbed, I wanted to get out of my chair and punch them in the head. Needless to say, this scared the shit out of me. What that person had been saying was just stupid and ignorant, but definitely not worthy of a physical altercation.
When this same rage erupted again (and several times after that), I made an appointment with a psychiatrist. I told him what happened and he said that anger, irritability, agitation, hostility, and aggression are known side effects of said medication.
“But why now, years later?”
He didn’t really give me a satisfying answer. Just waved his hand dismissively in the air and said, “it’s called tachyphylaxis or in laymen’s terms, breakthrough depression. Over time the brain adapts to your medication, you develop a tolerance, maybe there’s a change in your stress factors, or metabolic changes. You are getting older after all. Or you’ve got an untreated underlying mental illness that previous doctors hadn’t uncovered before.”
Thanks for that, doc.
“Don’t worry, the good news is there are many new medications available these days.” He said this last bit as if I’d still been taking aspirin years after Tylenol had been invented.
Damn, this guy was annoying. But not as bad as the other psychs I’d been to. Ones that looked down at me as if I was some sort of unclassified species. Addict-erectus. As he yammered on, about who-knows-what (at this point in the conversation I’d stopped listening), I felt my adrenaline rise to a boiling point, as my self-esteem simultaneously deflated into nonexistence. I was stuck between an oncoming homicidal rage and my normal abject introverted depression. Dreading the outcome with either of them I simply said, “I’ll give it ago.” If there is one thing about being a drug addict, even one that’s not actively using, I’m always up for a new drug to fix whatever ails me.
Are you saying a pill will fix this? Hand that shit over.
What my psychiatrist prescribed was a double whammy medication approach. A newer SSRI antidepressant that promised to address my anxiety as well as my depression. And because I wasn’t really sleeping anymore, he had an oldie but a goodie up his sleeve, a noradrenergic and specific serotonergic antidepressant (NaSSA) that can be used “off-label” to help with insomnia due to its sedative antihistamine properties.
For a former heroin addict, the idea of real sleep was very inviting. For years, I’d been getting four-to-five hours a night. I was totally exhausted, and never felt rested. I chalked it up to getting on in years. Everyone knows old folks don’t sleep. I’d been pounding melatonin as a “cure,” but apparently the amount I was taking wasn’t good for my brain chemistry either—causing a hormone overload—and there I was again, taking massive amounts of a substance, the body naturally manufactures, and throwing my neuroendocrine system all out of whack.
“Okay,” I said. While inexplicably perturbed with the prospect of having to take a pill in the morning and another at night. But then, you know, maybe I was more messed up than I thought. I was, after all, fanaticizing about losing my shit and going full MMA on people for very mundane reasons.
Within two weeks of taking these new drugs my sex drive became non-existent and my appetite increased. A month later I had packed on five pounds. I was constantly fatigued and my dreams were vivid, frantic, and bordering on nightmares. I didn’t like how I felt and immediately wanted off the meds (weight gain being a definite problem with my somewhat dormant eating disorder). But my psychiatrist cautioned me to wait for the medications to take full effect (at least 30 days), and besides, he warned, there were “adverse” reactions should I abruptly stop taking them.
Every morning I’d wake up soaked in sweat, my covers tangled around me as if I’d been fighting to get out of them. I went online and searched the drug’s side effects (my advice on this, don’t do it. You’ll self-diagnose yourself into a malignant tumor or some obscure terminal disease). Turns out I was the reigning archetype for all these drugs’ adverse reactions. I told my psychiatrist I didn’t like the meds, especially the sleep medication—my dreams were too intense, I was beyond groggy in the morning, and I was getting to be a bit of a pudge. He suggested I stay on the antidepressant (who needs a libido) and switch to a non-controlled “sedative” medication used to treat insomnia (really just a glorified antihistamine).
As soon as I got off the sleep meds I was back to being up all night—the antihistamine doing shit all nothing. Meanwhile, due to the antidepressant’s side effects, if I even slightly attempted any physical exertion (walk up a flight of stairs, etc.), I would sweat profusely (like the proverbial pig) my clothes soaked through with perspiration. I felt like I was ninety years old, with aches and pains and a foggy brain, especially first thing in the morning.
Hey doc, have the drugs taken full effect yet?
“The meds aren’t t working,” I told the psychiatrist. It had been three long uncomfortable months.
“Well, we gave it a try,” he said. His use of the word “we” really pissed me off. “Okay, how about we try an SNRI. They’ve been having really great results with depressives.” He followed that with listing off several names of drugs I’d never heard of.
Did this fool just call me a depressive?
“Whatever you think?” I said. He was the psychiatrist after all. I didn’t know a Pristiq from a Lexapro from a Trintellix. The mechanism of a SSRI compared to a SNRI or even what the hell a NDRI did. I really didn’t care what inhibited or blocked the reuptake, or what the hell it was even reuptaking.
Just give me something that fuckin’ works.
“And for the sleep, I’m prescribing a melatonin receptor agonist. It’s used to treat insomnia.”
The SNRI looked kind of promising. The known side effects were the usual nausea, dizziness, insomnia, sweating, and constipation; with the assurance that they go away with time as the body and mind accepted this new chemical balance.
The process of switching antidepressants is called titrating, “gradually adjusting a medication dose—increasing or decreasing it over time—to find the minimum effective amount that provides maximum benefit while minimizing side effects.” Well, that’s the theory, anyway. For two weeks I take half a dose of the old med, and half a dose of the new meds. Then stop the old one, and go full dose on the new one. In the interim, I feel a bit spaced out, but nothing I can’t deal with. Unfortunately, I’m also experiencing a bit of blunting—“a reduced ability to feel positive and negative emotions.” Often described as an emotional detachment, or a sense of indifference. In other words, no joy, no depression. Just flatlining through life. And… the excessive sweating is back.
Sleep however, is also not good. The new antidepressant keeps me awake. The melatonin receptor agonist works sometimes. Other nights I just lay in bed wide-awake. When I do get sleep, it’s only for five hours, and I wake up plagued with urgent obsessive thoughts about things I’m already going to do. Feed the cats, man. Feed the goddamn cats. Dude, the cats are starving. Feed them! When all my joints begin to ache with an arthritic dull pain (another known side effect), I call it quits.

The psychiatrist is visibly annoyed. Abruptly suggests another SNRI. I say, “I’ll take it.” Avoiding an additional lecture on the mechanics of said medication, and moving this drudgery of another medication taper along.
What kinda bullshit drug takes a month to work?
Almost immediately, things go even more south. I have never been suicidal. Outside of putting a gun to my head, many years ago, when my drug addiction had run its course into oblivion; my best friend had been murdered, I was wanted by the police, and I just couldn’t do the hustle for drugs anymore. Checking out felt like a good idea. Yet even in that defeated mental state I couldn’t go through with it—I just didn’t have it in me. I’m just not a suicidal guy (definitely more the homicidal type, ya know).
But this new antidepressant has me on the ropes. I’m so down everything looks like up. I’m haunted by dark thoughts. I’m plagued by what I think others are thinking. I obsessed with the desire to trace the edge of the desk onto a piece of paper. But, I couldn’t even tell you why or what I needed to do that for. If something moves, I have to look at it. Graphic thoughts of other people’s sex lives come and go; do they do this, or that? People I wouldn’t normally contemplate anything about, let alone their intimate details. When I’m driving, I fanaticize of steering my car into oncoming traffic, or undoing my seatbelt and just pushing down the accelerator and slamming into a concrete wall. None of these thoughts feel wrong, or off, or that I shouldn’t be having them. But in the back of my mind, like an observer, I’m thinking, What the actual fuck is going on?
I call the psychiatrist. He doesn’t get back to me. I email the psychiatrist. Nothing. I stop taking the pills. The black cloud disappears. But the damage has been done. My confidence is at an all-time low. Self-esteem is none existent. I feel like a fraud going into work and helping clients get back on their feet and heal. I’m no better than they are, except I’m not using drugs, and most of them are on some form of psychiatric medication.
Why doesn’t this shit work for me?
The withdrawal is brutal. I experienced “brain zaps,” little pings to my brain that feel electric; popping out of nowhere, at random, whenever they want. A vacant void of emotions mixed with the most overwhelming introverted feelings. Was this better than wanting to kill myself? I guess I’d have to say yes.
A week later the psychiatrist sets up a video visit. Possibly he knew I wasn’t someone he physically wanted to be in a room with. “So, how’s it going?”
“I stopped taking the pills. I wanted to kill myself.”
“Hey, don’t be so dramatic.” I’m not sure which one he considers dramatic. That I was suicidal, or I stopped the medication.
I tell the doctor I want to go back on the original NDRI. I’m figuring homicidal rage beats suicide any day. He suggests another drug, a serotonin modulator and stimulator (SMS), but I just can’t fathom going through the ups and downs of a trying one more damn drug—the “what if it doesn’t work?” haunting me like the shrouded specter of abject fear.
“The NDRI doesn’t do anything for your anxiety.”
“Neither does all this.”
I start out on the lowest dose possible of the original antidepressant. My anxiety immediately goes through the roof. I’m functioning as best I can. But this isn’t the answer. I mistake people’s reactions and words as criticism. Someone laughs, and I know it’s about me. The idea of leaving the house, feels intimidating. I’m in a grocery store, pushing my cart, avoiding eye contact and a woman yells my name. I’m not even sure who she is, but she hugs me, in a way that implies we’re friends.
Have I finally lost my grip on reality?
I go home and toss the antidepressant in the trash. Call my psychiatrist and leave a message, “you’re right, my anxiety’s the issue. I can deal with the depression.”
He prescribes a partial agonist of the serotonin receptor that, “impacts serotonin activity to reduce anxiety.” Almost immediately, like a mental placebo, my anxiety somewhat subsides. I’m also back on the originally prescribed sleep meds. This time, without any interactions with an antidepressant, I don’t have the crazy dreams or night sweats. I’m sleeping. I’m breathing—with eight hours of sleep I’m as composed as I can get.
I’m also somewhat back on my daily routine; meditation, exercise, caffeine and a healthy diet. Although the coffee part can trigger an episode of anxiety (I just have to not over indulge), I am, for the most part, okay. Moments, like this morning, where I was distressed about nothing I could really explain, appear out of nowhere. Yesterday was relatively routine until I had to venture out into the world and deal with people—my social anxiety at an all-time high. Yet the day before, all was good and I felt confident and capable. So, I guess it’s safe to say that I am back to “normal.” I have good days, and bad days. For the most part, I don’t want to punch stupid people in the head, blow my brains out, or hide under the duvet. It’s just the usual chemical business up here in my brain.
At least for now.